Despite the amount of research performed, the cost-effectiveness of direct oral anticoagulants (DOACs) in subpopulations with different risk factors for stroke has been very little studied. This study aims to explore the cost-effectiveness of the DOACs available in Malaysia in preventing stroke in different subpopulations from a government perspective. An existing Markov model was adapted to assess the cost-effectiveness of the DOACs that are available in Malaysia namely, apixaban (AP), dabigatran (DA) and rivaroxaban (RV). Each was compared with vitamin K antagonists (VKA) in stroke prevention in different patient subpopulations including chronic kidney disease (CKD), high-age, diabetes (DM), and prolonged hospital stay. Cost-effectiveness was assessed by the incremental cost-effectiveness ratio (ICER) benchmarked against the local threshold for cost-effectiveness. The total cost of VKA, AP, DA and RV was Malaysian Ringit (RM) RM9,811 (1USD=RM4.76), RM16,858, RM18,318 and RM20,161 respectively. The quality adjusted life-years (QALYs) gained compared with VKA were 6.11, 6.09 and 6.15 respectively. The ICER when compared with VKA at base case was 57,539, -90,682 and 68,156 respectively. AP had the most favourable ICER at base case. RV had the best ICER compared to AP and DA in patients with CKD and DM at a willingness-to-pay threshold of 1-GDP. Probabilistic sensitivity analysis showed that RV was consistently the most favourable DOAC under a threshold of 2-GDP for all subpopulations. These findings suggested that rivaroxaban has the most favourable ICER in the CKD and DM patient subgroups for stroke prevention among the DOACs available in Malaysia at a threshold of 2-GDP.
| Published in | International Journal of Health Economics and Policy (Volume 9, Issue 1) |
| DOI | 10.11648/j.hep.20240901.12 |
| Page(s) | 19-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Stroke Prevention, Direct Oral Anticoagulants, Cost-Effectiveness, Diabetes, Chronic Kidney Disease, Threshold, QALY
Value | Range in DSA | Distribution in PSA | Refer-ences | |
|---|---|---|---|---|
Clinical values | ||||
Pr major stroke - Rivaroxaban | 0.227% | (0.21%, 0.24%) | Beta (819, 360,359) | 16 |
Pr minor stroke - Rivaroxaban | 0.072% | (0.07%, 0.08%) | Beta (821, 1,138,660) | 16 |
Pr Myocardial infarction - Rivaroxaban | 0.225% | (0.2%, 0.25%) | Beta (280, 124,175) | 16 |
Pr GI Bleed - Rivaroxaban | 0.687% | (0.64%, 0.74%) | Beta (694, 100,280) | 16 |
Pr ICH - Rivaroxaban | 0.333% | (0.3%, 0.37%) | Beta (444, 132,953) | 16 |
Pr major stroke - Dabigatran | 0.221% | (0.2%, 0.24%) | Beta (538, 243,383) | 16 |
Pr minor stroke - Dabigatran | 0.070% | (0.06%, 0.08%) | Beta (539, 768,976) | 16 |
Pr Myocardial infarction - Dabigatran | 0.254% | (0.22%, 0.3%) | Beta (192, 75,285) | 16 |
Pr GI Bleed - Dabigatran | 0.636% | (0.57%, 0.7%) | Beta (398, 62,145) | 16 |
Pr ICH - Dabigatran | 0.313% | (0.19%, 0.22%) | Beta (252, 80,144) | 16 |
Pr major stroke - Apixaban | 0.202% | (0.06%, 0.07%) | Beta (650, 320,870) | 16 |
Pr minor stroke - Apixaban | 0.064% | (0.23%, 0.25%) | Beta (650, 1,013,536) | 16 |
Pr Myocardial infarction - Apixaban | 0.240% | (0%, 0%) | Beta (1600, 665,788) | 16 |
Pr GI Bleed - Apixaban | 0.489% | (0.25%, 0.32%) | Beta (444, 90,300) | 16 |
Pr ICH - Apixaban | 0.279% | (0.19%, 0.22%) | Beta (311, 111,339) | 16 |
Pr major stroke - VKA | 0.311% | (0.3%, 0.32%) | Beta (5613, 1,801,672) | 16 |
Pr minor stroke - VKA | 0.099% | (0.1%, 0.1%) | Beta (5625, 5,699,430) | 16 |
Pr Myocardial infarction - VKA | 0.240% | (0.23%, 0.25%) | Beta (1600, 665,788) | 16 |
Pr GI Bleed - VKA | 0.568% | (0.56%, 0.58%) | Beta (10739, 1,878,734) | 16 |
Pr ICH - VKA | 0.387% | (0.38%, 0.4%) | Beta (6725, 1,732,154) | 16 |
Probability of mortality from major stroke | 25.57% | (25.09%, 26.05%) | Beta (7996, 23,276) | 16 |
Probability of mortality from GI bleed | 14.63% | (13.74%, 15.52%) | Beta (882, 5,147) | 16 |
Probability of mortality from Post-major stroke | 8.12% | (7.35%, 8.92%) | Beta (390, 4,410) | 16 |
Probability of mortality from Post IC bleed | 14.11% | (11.85%, 16.57%) | Beta (128, 781) | 16 |
Probability of mortality from ICH | 28.50% | (24.23%, 32.78%) | Beta (122, 306) | 16 |
Probability of mortality from MI | 24.67% | (23.79%, 25.55%) | Beta (2257, 6,893) | 16 |
Probability of mortality from Post-MI | 8.24% | (7.17%, 9.34%) | Beta (211, 2,347) | 16 |
Utility values | ||||
Stable AF | 0.80 | (0.78, 0.82) | Beta (1425, 361) | 17 |
Minor IS | 0.67 | (0.57, 0.77) | Beta (56, 28) | 18 |
Major IS | 0.38 | (0.32, 0.44) | Beta (56, 28) | 18 |
Post minor IS | 0.67 | (0.57, 0.77) | Beta (105, 172) | 18 |
Post major IS | 0.56 | (0.48, 0.64) | Beta (75, 59) | 18 |
GI bleeding | 0.70 | (0.60, 0.81) | Beta (51, 22) | 20 |
IC bleeding | 0.56 | (0.48, 0.64) | Beta (75, 59) | 18 |
Post IC bleeding | 0.67 | (0.57, 0.77) | Beta (56, 27) | 18 |
MI | 0.72 | (0.61, 0.83) | Beta (46, 18) | 19 |
Post MI | 0.80 | (0.68, 0.92) | Beta (34, 9) | 19 |
Cost (RM) | ||||
Rivaroxaban daily cost | 6.74 | (5.06, 8.43) | Gamma (61, 0.11) | MI* |
Dabigatran daily cost | 6.84 | (5.13, 8.55) | Gamma (61, 0.11) | MI* |
Apixaban daily cost | 6.54 | (4.91, 8.18) | Gamma (61, 0.11) | MI* |
VKA daily cost | 0.39 | (0.29, 0.49) | Gamma (61, 0.01) | 24 |
Acute Treatment - minor | 3,224 | (2,418, 4,030) | Gamma (61, 52) | 8 |
Acute Treatment - major | 4,571 | (3,428, 5,714) | Gamma (61, 74) | 8 |
Follow up costs - Minor (per cycle) | 534 | (336, 777) | Gamma (200, 3) | 8 |
Follow up costs - Major (per cycle) | 1,134 | (572, 1,884) | Gamma (102, 11) | 8 |
Rehabilitation Costs | 418 | (314, 523) | Gamma (61, 7) | 22 |
Acute Treatment | 19,381 | (14,536, 24,227) | Gamma (61, 315) | 21 |
Follow up costs - MI (per cycle) | 474 | (391, 564) | Gamma (8, 60) | 21 |
Acute Treatment - GI bleed | 5,876 | (4,407, 7,345) | Gamma (61, 96) | 22 |
Acute Treatment - IC bleed | 10,749 | (8,062, 13,436) | Gamma (61, 175) | 22 |
Follow up costs - Bleeds | 1,469 | (572, 1,884) | Gamma (1138, 1) | 22 |
Rehabilitation Costs | 261 | (196, 326) | Gamma (61, 4) | 23 |
Treatment | Total Costs (RM) (95% CI) | Total QALYs (95% CI) | ICERs vs VKA |
|---|---|---|---|
Base-case scenario | |||
VKA | 9,811 (8,973; 10,704) | 5.98 (5.88; 6.08) | - |
Apixaban | 16,858 (14,582; 19,484) | 6.11 (6.00; 6.22) | 57,539 |
Dabigatran | 18,318 (15,667; 21,665) | 6.09 (5.97; 6.22) | (Dominated) |
Rivaroxaban | 20,161 (17,329; 23,453) | 6.15 (6.05; 6.27) | 68,156 |
Sub-population with moderate to severe CKD stage 3-5 | |||
VKA | 14,931 (9,471; 11,242) | 4.46 (5.68; 5.9) | - |
Apixaban | 21,193 (15,254; 20,096) | 4.84 (5.74; 6.02) | 16,316 (Extendedly dominated)* |
Dabigatran | 21,774 (15,502; 21,618) | 4.87 (5.71; 6.06) | 16,474 (Extendedly dominated) |
Rivaroxaban | 23,564 (17,566; 23,839) | 5.05 (5.90; 6.15) | 14,433 |
Sub-population with age > 85 years old | |||
VKA | 14,367 (13,218; 15,625) | 4.68 (4.57; 4.79) | - |
Apixaban | 20,640 (18,374; 23,229) | 5.01 (4.80; 5.21) | 19,351 |
Dabigatran | 21,984 (19,463; 25,055) | 4.85 (4.69; 5.01) | (Dominated) |
Rivaroxaban | 23,284 (20,541; 26,388) | 5.09 (4.94; 5.24) | 31,739 |
Sub-population with diabetes | |||
VKA | 10,318 (8,973; 10,704) | 5.79 (5.88; 6.08) | - |
Apixaban | 17,538 (14,582; 19,484) | 5.88 (6.00; 6.22) | 78,880 (Extendedly dominated) |
Dabigatran | 18,170 (15,667; 21,665) | 5.87 (5.97; 6.22) | (Dominated) |
Rivaroxaban | 20,544 (17,329; 23,453) | 6.03 (6.05; 6.27) | 42,948 |
Length of stay (LOS) | Average LOS | ||
VKA | 9,811 (8,954; 10,692) | 0.27 (0.27; 0.27) | |
Apixaban | 16,858 (14,597; 19,521) | 0.17 (0.18; 0.15) | 69,040 |
Dabigatran | 18,318 (15,578; 21,600) | 0.16 (0.18; 0.14) | 243,022 (Extendedly dominated) |
Rivaroxaban | 20,161 (17,304; 23,423) | 0.14 (0.14; 0.14) | 112,981 |
AF | Atrial Fibrillation |
NVAF | Non-Valvular Atrial Fibrillation |
DOAC | Direct Oral Anticoagulant |
VKA | Vitamin K Antagonists |
LMWHs | Low Molecular-weight Heparins |
RWE | Real-World Evidence |
RV | Rivaroxaban |
AP | Apixaban |
DA | Dabigatran |
CKD | Chronic Kidney Disease |
DM | Diabetes Mellitus |
QALYs | Quality Adjusted life Years |
IS | Ischemic Stroke |
MI | Myocardial Infarction |
ICH | Intracranial Haemorrhage |
GI | Gastrointestinal |
DSA | Deterministic Sensitivity Analysis |
PSA | Probabilistic Sensitivity Analysis |
Pr | Probability |
ICER | Incremental Cost-Effectiveness Ratio |
WHO | World Health Organisation |
GDP | Gross Domestic Product |
WTP | Willingness-to-Pay |
HRs | Hazard Ratios |
EQ-5D | EuroQol-5 Dimension |
LOS | Length of Stay |
CE | Cost Effectiveness |
CEAC | Cost-Effectiveness Acceptability Curve |
ESRD | End-Stage Renal Disease |
CHEERS 2022 | Consolidated Health Economic Evaluation Reporting Standards 2022 |
Below is the link to the supplementary material:
| [1] | Feigin, V. L., B. Norrving, and G. A. Mensah, Global Burden of Stroke. Circ Res, 2017. 120(3): p. 439-448. |
| [2] | Sacco, R. L., et al., An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke, 2013. 44(7): p. 2064-89. |
| [3] | Lip, G. Y. H., C. M. Brechin, and D. A. Lane, The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe. Chest, 2012. 142(6): p. 1489-1498. |
| [4] | Ovbiagele, B., et al., Forecasting the future of stroke in the United States: a policy statement from the American Heart Association and American Stroke Association. Stroke, 2013. 44(8): p. 2361-75. |
| [5] | Malaysia Country Profile. Institute for Health Metrics and Evaluation. |
| [6] | Rose, D. K. and B. Bar, Direct Oral Anticoagulant Agents: Pharmacologic Profile, Indications, Coagulation Monitoring, and Reversal Agents. J Stroke Cerebrovasc Dis, 2018. 27(8): p. 2049-2058. |
| [7] | Choi, J. H., et al., Cost-effectiveness of Direct Oral Anticoagulant vs. Warfarin Among Atrial Fibrillation Patients With Intermediate Stroke Risk. Front Cardiovasc Med, 2022. 9: p. 849474. |
| [8] | Azahar, S. N., et al., Direct Medical Cost of Stroke and the Cost-Effectiveness of Direct Oral Anticoagulants in Atrial Fibrillation-Related Stroke: A Cross-Sectional Study. Int J Environ Res Public Health, 2022. 19(3). |
| [9] | Cervantes, C. E., J. L. Merino, and V. Barrios, Edoxaban for the prevention of stroke in patients with atrial fibrillation. Expert Rev Cardiovasc Ther, 2019. 17(4): p. 319-330. |
| [10] | Wei, H., et al., Cost-effectiveness analysis of dabigatran, rivaroxaban and warfarin in the prevention of stroke in patients with atrial fibrillation in China. BMC Health Serv Res, 2021. 21(1): p. 96. |
| [11] | Li, Y., et al., Methods for Economic Evaluations of Novel Oral Anticoagulants in Patients with Atrial Fibrillation: A Systematic Review. Appl Health Econ Health Policy, 2024. 22(1): p. 33-48. |
| [12] | Single Technology Appraisal (STA) of Rivaroxaban (Xarelto®). 2011, National Institute for Health and Clinical Excellence. |
| [13] | Pharmacoeconomic Guidline for Malaysia Second Edition. 2019, Ministry of Health Malaysia. |
| [14] | GDP per capita (current US$). 2022, The World Bank. |
| [15] | Lim, Y. W., et al., Determination of Cost-Effectiveness Threshold for Health Care Interventions in Malaysia. Value Health, 2017. 20(8): p. 1131-1138. |
| [16] | Grymonprez, M., et al., Long-term comparative effectiveness and safety of dabigatran, rivaroxaban, apixaban and edoxaban in patients with atrial fibrillation: A nationwide cohort study. Front Pharmacol, 2023. 14: p. 1125576. |
| [17] | Luengo-Fernandez, R., et al., Quality of life after TIA and stroke: ten-year results of the Oxford Vascular Study. Neurology, 2013. 81(18): p. 1588-95. |
| [18] | Pockett, R. D., et al., Health Utility in Patients Following Cardiovascular Events. Value Health, 2014. 17(7): p. A328. |
| [19] | Sullivan, P. W., et al., Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making, 2011. 31(6): p. 800-4. |
| [20] | Radaideh, K. M. and L. M. Matalqah, Health-Related Quality of Life among Atrial fibrillation Patients Undergoing Anticoagulation Therapy. Epidemiology, Biostatistics, and Public Health, 2022. 15(1). |
| [21] | Shafie, A. A. and C. H. Ng, Estimating the Costs of Managing Complications of Type 2 Diabetes Mellitus in Malaysia. Malaysian Journal of Pharmaceutical Sciences, 2020. 18(2): p. 15-32. |
| [22] | George, D., et al., Severity and hospitalization cost related to warfarin-related adverse events in a tertiary Malaysian hospital. Hosp Pharm, 2022. 57(5): p. 633-638. |
| [23] | Akhavan Hejazi, S. M., et al., Cost of post-stroke outpatient care in Malaysia. Singapore Med J, 2015. 56(2): p. 116-9. |
| [24] | Tan, S. K., W. L. Looi, and H. Y. Yeo, Estimation of direct medical costs of warfarin, dabigatran and rivaroxaban treatments in non‐valvular atrial fibrillation patients in a tertiary public hospital, Malaysia. Journal of Pharmacy Practice and Research, 2020. 50(5): p. 406-412. |
| [25] | Chan, Y. H., et al., Effectiveness, safety, and major adverse limb events in atrial fibrillation patients with concomitant diabetes mellitus treated with non-vitamin K antagonist oral anticoagulants. Cardiovasc Diabetol, 2020. 19(1): p. 63. |
| [26] | Goto, S., et al., Management and 1-Year Outcomes of Patients With Newly Diagnosed Atrial Fibrillation and Chronic Kidney Disease: Results From the Prospective GARFIELD - AF Registry. J Am Heart Assoc, 2019. 8(3): p. e010510. |
| [27] | Tsai, C. T., et al., Non-vitamin K antagonist oral anticoagulants versus warfarin in AF patients >/= 85 years. Eur J Clin Invest, 2021. 51(6): p. e13488. |
| [28] | El Kadri, M., et al., Patient characteristics, adherence, and costs of oral anticoagulation therapy in non-valvular atrial fibrillation using the Dubai Real-World Claims Database. Avicenna J Med, 2021. 11(2): p. 93-102. |
| [29] | Wyld, M. and A. C. Webster, Chronic Kidney Disease is a Risk Factor for Stroke. J Stroke Cerebrovasc Dis, 2021. 30(9): p. 105730. |
| [30] | Time series population projection by ethnic group, sex and state. 2017, Department of Statistics Malaysia. |
| [31] | Ganasegeran, K., et al., A Systematic Review of the Economic Burden of Type 2 Diabetes in Malaysia. Int J Environ Res Public Health, 2020. 17(16). |
| [32] | Husereau, D., et al., Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) Statement: Updated Reporting Guidance for Health Economic Evaluations. Value Health, 2022. 25(1): p. 3-9. |
APA Style
Lee, K. K., Zheng, C., Lim, J., Choon, J. W. (2024). Cost-Effectiveness of Rivaroxaban Compared with Other Direct Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation in Public Sector of Malaysia. International Journal of Health Economics and Policy, 9(1), 19-29. https://doi.org/10.11648/j.hep.20240901.12
ACS Style
Lee, K. K.; Zheng, C.; Lim, J.; Choon, J. W. Cost-Effectiveness of Rivaroxaban Compared with Other Direct Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation in Public Sector of Malaysia. Int. J. Health Econ. Policy 2024, 9(1), 19-29. doi: 10.11648/j.hep.20240901.12
AMA Style
Lee KK, Zheng C, Lim J, Choon JW. Cost-Effectiveness of Rivaroxaban Compared with Other Direct Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation in Public Sector of Malaysia. Int J Health Econ Policy. 2024;9(1):19-29. doi: 10.11648/j.hep.20240901.12
@article{10.11648/j.hep.20240901.12,
author = {Kenneth Kwing-Chin Lee and Charles Zheng and Jing-Sheng Lim and June Wai-Yee Choon},
title = {Cost-Effectiveness of Rivaroxaban Compared with Other Direct Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation in Public Sector of Malaysia
},
journal = {International Journal of Health Economics and Policy},
volume = {9},
number = {1},
pages = {19-29},
doi = {10.11648/j.hep.20240901.12},
url = {https://doi.org/10.11648/j.hep.20240901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.hep.20240901.12},
abstract = {Despite the amount of research performed, the cost-effectiveness of direct oral anticoagulants (DOACs) in subpopulations with different risk factors for stroke has been very little studied. This study aims to explore the cost-effectiveness of the DOACs available in Malaysia in preventing stroke in different subpopulations from a government perspective. An existing Markov model was adapted to assess the cost-effectiveness of the DOACs that are available in Malaysia namely, apixaban (AP), dabigatran (DA) and rivaroxaban (RV). Each was compared with vitamin K antagonists (VKA) in stroke prevention in different patient subpopulations including chronic kidney disease (CKD), high-age, diabetes (DM), and prolonged hospital stay. Cost-effectiveness was assessed by the incremental cost-effectiveness ratio (ICER) benchmarked against the local threshold for cost-effectiveness. The total cost of VKA, AP, DA and RV was Malaysian Ringit (RM) RM9,811 (1USD=RM4.76), RM16,858, RM18,318 and RM20,161 respectively. The quality adjusted life-years (QALYs) gained compared with VKA were 6.11, 6.09 and 6.15 respectively. The ICER when compared with VKA at base case was 57,539, -90,682 and 68,156 respectively. AP had the most favourable ICER at base case. RV had the best ICER compared to AP and DA in patients with CKD and DM at a willingness-to-pay threshold of 1-GDP. Probabilistic sensitivity analysis showed that RV was consistently the most favourable DOAC under a threshold of 2-GDP for all subpopulations. These findings suggested that rivaroxaban has the most favourable ICER in the CKD and DM patient subgroups for stroke prevention among the DOACs available in Malaysia at a threshold of 2-GDP.
},
year = {2024}
}
TY - JOUR T1 - Cost-Effectiveness of Rivaroxaban Compared with Other Direct Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation in Public Sector of Malaysia AU - Kenneth Kwing-Chin Lee AU - Charles Zheng AU - Jing-Sheng Lim AU - June Wai-Yee Choon Y1 - 2024/08/20 PY - 2024 N1 - https://doi.org/10.11648/j.hep.20240901.12 DO - 10.11648/j.hep.20240901.12 T2 - International Journal of Health Economics and Policy JF - International Journal of Health Economics and Policy JO - International Journal of Health Economics and Policy SP - 19 EP - 29 PB - Science Publishing Group SN - 2578-9309 UR - https://doi.org/10.11648/j.hep.20240901.12 AB - Despite the amount of research performed, the cost-effectiveness of direct oral anticoagulants (DOACs) in subpopulations with different risk factors for stroke has been very little studied. This study aims to explore the cost-effectiveness of the DOACs available in Malaysia in preventing stroke in different subpopulations from a government perspective. An existing Markov model was adapted to assess the cost-effectiveness of the DOACs that are available in Malaysia namely, apixaban (AP), dabigatran (DA) and rivaroxaban (RV). Each was compared with vitamin K antagonists (VKA) in stroke prevention in different patient subpopulations including chronic kidney disease (CKD), high-age, diabetes (DM), and prolonged hospital stay. Cost-effectiveness was assessed by the incremental cost-effectiveness ratio (ICER) benchmarked against the local threshold for cost-effectiveness. The total cost of VKA, AP, DA and RV was Malaysian Ringit (RM) RM9,811 (1USD=RM4.76), RM16,858, RM18,318 and RM20,161 respectively. The quality adjusted life-years (QALYs) gained compared with VKA were 6.11, 6.09 and 6.15 respectively. The ICER when compared with VKA at base case was 57,539, -90,682 and 68,156 respectively. AP had the most favourable ICER at base case. RV had the best ICER compared to AP and DA in patients with CKD and DM at a willingness-to-pay threshold of 1-GDP. Probabilistic sensitivity analysis showed that RV was consistently the most favourable DOAC under a threshold of 2-GDP for all subpopulations. These findings suggested that rivaroxaban has the most favourable ICER in the CKD and DM patient subgroups for stroke prevention among the DOACs available in Malaysia at a threshold of 2-GDP. VL - 9 IS - 1 ER -
School of Medicine and Health Sciences, Monash University Malaysia, Selangor, Malaysia; School of Pharmacy, Faculty of Health and Medical Sciences, Taylor's University, Selangor, Malaysia
Biography: Kenneth Kwing-Chin Lee is Professor of Health Economics at School of Medicine, Monash University Malaysia. He obtained his undergraduate degree in pharmacy from the University of Washington in Seattle, USA. His subsequent higher qualifications were from the Chinese University of Hong Kong and the University of Oxford, UK. Prof Lee is widely recognized as one of the pioneers in health economics and outcomes research in Asia. He has been Editor-in-chief of Journal of Medical Economics since 2006 and Topic Editor of “Increasing Importance of Patients-generated Real-World Data for Healthcare Policy Decisions about Medicinal Products” of Frontiers in Pharmacology since 2020. His areas of specialty include both micro and macro health economics. He had worked on individual drug therapies and surgical procedures as well as healthcare policy. He had been advisor of several Malaysia government committees including the Pharmacoeconomics Guideline Advisory Committee and Drug Pricing Control Committee.
Research Fields: Health technology assessment, Health policy research, Cost-effectiveness analysis of pharmaceuticals, Indirect cost of cancer patients, Equity to access healthcare

School of Pharmacy, Faculty of Health and Medical Sciences, Taylor's University, Selangor, Malaysia
Biography: Charles Zheng is a Staff Member of Cochrane Singapore. He acquired his degree in Preventive Medicine from Shanghai Jiao Tong University in 2012, and his Master of Philosophy in Public Health from The University of Hong Kong and Master of Science in Health Technology Assessment from University of York in 2014 and 2019, respectively. His major research interests lie in health economic modelling, real-world study and systematic reviews.
Research Fields: Health economics, Health technology assessment, Epidemiology, Biostatistics, Real-World Evidence

School of Pharmacy, Faculty of Health and Medical Sciences, Taylor's University, Selangor, Malaysia
Biography: Jing-Sheng Lim is a PhD candidate at the School of Pharmacy, Taylor's University. He obtained his Bachelor of Pharmacy (Hons) from the same institution and subsequently commenced a Master of Philosophy in Pharmacy before transitioning to his current doctoral studies. In recognition of his outstanding contributions, he was awarded the National MPS Excellence Award 2024 by the Malaysian Pharmacists Society. Mr. Lim actively contributes to the pharmaceutical and healthcare community through various leadership roles. He is a member of the steering committee of the Malaysian Young Pharmacists Chapter and serves as the Chairperson of the Malaysian Innovative Healthcare Symposium. His engagement in the field includes participation in numerous discussions with international health economists, policy stakeholders, and industry experts. Additionally, he is a member of ISPOR and the ISPOR Asia Consortium.
Research Fields: Health technology assessment, Economic burden of disease (direct and indirect cost), Oncology, Health policy research, Equity to access healthcare

Centre for Drug Policy and Health Economic Research (CDPHER), University Teknologi MARA (UiTM), Selangor, Malaysia
Biography: June Wai-Yee Choon is a Senior Lecturer at Faculty of Pharmacy, Universiti Teknologi MARA. With her expertise in Health Economics and Outcomes Research, and academic experience spanning the UK (University of Cardiff), Australia (Monash University Malaysia) and Malaysia (UiTM, Puncak Alam), Dr Choon has held pivotal roles in various national level steering committees such as the National Committee for Clinical Research (NCCR), Ministry of Health and advisory roles for the pharmaceutical industry. Known for her roles in bridging academia with the Ministry of Health and pharmaceutical industry, she is passionate about driving positive change and interdisciplinary initiatives in improving patient access to innovative medicines in Malaysia.
Research Fields: Health Economics, Healthcare Financing, Healthcare Policy, Real-World Evidence

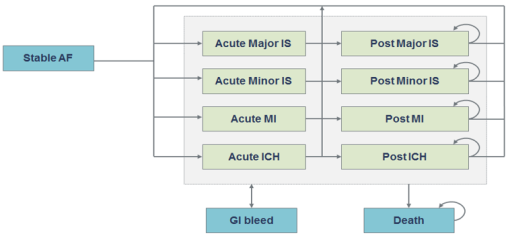
Figure 1. Schematic illustration of model. The model comprises a series of health states based on potential complications of NVAF (stable AF, acute and post-major IS, acute and post-minor IS, acute and post-MI, acute and post-ICH and GI bleed), and the absorbing state of death. Patients on VKA and each of the studied DOACs were transit through the model in cycles of 3 months, accumulating QALYs associated with each health state, together with the costs of treatment, events, and subsequent monitoring.
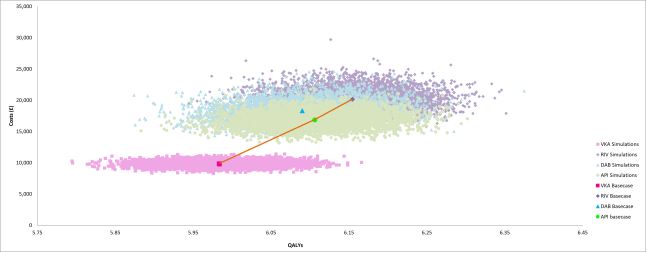
Figure 2. Cost Effectiveness (CE) plane for base-case population. The cost of VKA, AP, DA and RV was RM9,811, 16,858, 18,318 and 20,161 respectively (1USD=RM4.74).
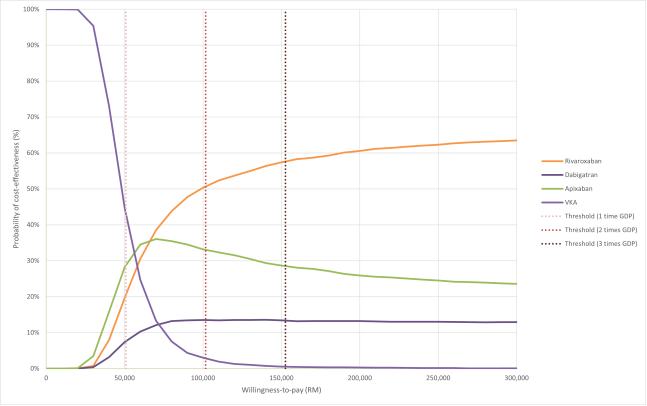
Figure 3. Cost-Effectiveness Acceptability Curve (CEAC) for base-case population. The ICER of AP was comparable to RV with DA dominated as compared with VKA with total QALYs gained for; AP=6.11; RV=6.15; DA=6.09 and VKA=5.98.

