Abstract
This research pinpoints the multifaceted barriers that influence health-care seeking behaviour in India. It addresses a critical gap in understanding why a significant portion of the population are not utilising healthcare despite many national health initiatives. The main purpose of this study is to investigate how financial means, geographical inaccessibility and a lack of faith in the medical system intersect and ultimately lead to the deterrence of individuals from seeking necessary medical treatment or interventions. The study aims to provide actionable insights and policy recommendations to refine the public health strategy in India. Utilising the National Health Survey (2017-2018), the research analyses a sample of 113,823 households. The analysis reveals interesting findings - (a) the poorest 20% are nearly three times more likely to avoid care due to lack of faith in the medical facilities compared to the richest 20%; (b) geographical distance is a primary deterrent with 27% of the respondents citing there is a lack of a nearby medical facility, hence avoiding treatment till it is absolutely vital; (c) Despite availability of policies to reduce the burden of healthcare expenses such as PM-JAY, the financial burden still remains high for many. These results highlight that expanding insurance coverage is insufficient without investments in rural infrastructure and other initiatives to rebuild public trust in the healthcare system.
Keywords
NHS 75th Round, Out-of-pocket Expenditure, Non-utilisation, Geographical Inaccessibility, Trust Deficit
1. Introduction
The healthcare infrastructure in India has expanded significantly over recent decades, characterised by a sustained increase in public health expenditure. Government health expenditure (GHE) as a proportion of the GDP rose from 1.15% in 2013-14 to approximately 1.84%-2.1% by 2022-23, while per capita health spending tripled from ₹1,108 in 2014-15 to ₹3,169 in 2021-22
. Furthermore, the share of government expenditure in total health spending increased considerably from 29% to 48% between FY2015 and FY2022, signalling a progressive shift away from out-of-pocket financing toward state-led provisioning of healthcare resources
. This fiscal expansion has been accompanied by the growth of both public and private medical facilities across urban and rural areas, broadening the overall availability of health services nationwide.
However, despite these improvements in the availability of health care services, a substantial proportion of the Indian population continues to forgo and ignore necessary medical treatment when ill or injured. This persistent pattern of healthcare non-utilisation brings our attention to a critical and widening gap between the supply-side expansion of health services and their actual consumption by the population: a disjunction that has significant implications for national health outcomes, economic productivity, and broader developmental goals.
The non-utilisation of healthcare services has profound consequences for both individual and population-level health outcomes. When individuals forgo or unduly delay medical attention, presenting conditions frequently progress to more advanced and clinically severe stages, substantially complicating the scope and cost of required intervention. This not only diminishes the efficacy of treatment but also places a considerably heightened financial burden upon affected households, particularly among lower-income groups who have limited capacity to absorb heightened medical expenditures. At the systemic level, the increased prevalence of advanced-stage illness intensifies demand pressures on an already strained public healthcare infrastructure, diverting finite clinical resources towards conditions that may have been managed at significantly lower cost had timely care been sought.
The implications of healthcare non-utilisation extend considerably beyond its immediate clinical consequences, exerting significant adverse effects on economic functioning and national development objectives. Untreated illness materially reduces labour force participation and productivity, with disproportionate consequences for working-age populations in labour-intensive sectors. At the household level, the convergence of diminished earnings and escalating medical expenditure deepens existing cycles of poverty among economically vulnerable groups, collectively constituting a substantive impediment to macroeconomic productivity and India's broader objective of Universal Health Coverage.
Existing literature on healthcare in India has predominantly focused on improving service quality and efficiency within hospitals and clinics: examining patient satisfaction, treatment protocols, and institutional performance after individuals have already accessed care. However, these bodies of research largely overlook the antecedent question: ‘Why do individuals fail to reach healthcare facilities in the first place, even when services are ostensibly available?’ This represents a significant analytical gap, as understanding the barriers to initial healthcare seeking behaviour is fundamental to addressing overall health system utilisation.
This study addresses this gap by conducting a comprehensive quantitative economic analysis of healthcare non-utilisation using data from the National Health Survey 2017-18. Drawing on approximately 150,000 observations, this research systematically examines the association between financial constraints and behavioural barriers and their influence on treatment-seeking decisions. The primary aim of this study is to identify the key determinants that prevent healthcare utilisation, and thereby provide evidence-based policy recommendations to guide a more efficient allocation of the government’s healthcare budget through targeted interventions that reduce barriers to care.
2. Background
Healthcare non-utilisation in India is a complex problem driven by financial constraints, behavioural determinants, and socio-demographic disparities. The corpus of empirical literature examining this domain reveals that healthcare access and utilisation patterns are profoundly stratified across income quintiles, geographic locations, and gender dimensions. Ghosh (2014) in
Equity in the utilisation of healthcare services in India: evidence from National Sample Survey demonstrates that wealthier individuals consistently use healthcare services more than poorer populations across Indian states, with financial capacity playing a decisive role in determining access, especially in rural settings. The study's rigorous analysis of horizontal inequities, predicated on health-needs standardisation, quantifies the extent of financial stratification in healthcare consumption across both outpatient and inpatient care, thereby confirming the premise that the ability to pay remains a critical factor determining whether people seek medical treatment.
| [1] | Ghosh S. (2014). Equity in the utilization of healthcare services in India: evidence from National Sample Survey. International journal of health policy and management, 2(1), 29–38.
https://doi.org/10.15171/ijhpm.2014.06 |
| [3] | Purohit B. C. (2004). Inter-state disparities in health care and financial burden on the poor in India. Journal of health & social policy, 18(3), 37–60. https://doi.org/10.1300/J045v18n03_03 |
[1, 3]
.
Interestingly, the role of health insurance mechanisms in reducing financial barriers presents counterintuitive empirical evidence. Prinja et al. (2019) in
Role of insurance in determining utilisation of healthcare and financial risk protection in India examined major insurance schemes like the Rashtriya Swasthya Bima Yojana using household survey data and found no meaningful link between having insurance and actually accessing more care or spending less out-of-pocket.
| [2] | Prinja, S., Bahuguna, P., Gupta, I., Chowdhury, S., & Trivedi, M. (2019). Role of insurance in determining utilization of healthcare and financial risk protection in India. PloS one, 14(2), e0211793. |
[2]
Sinha and Chatterjee (2014) in
Assessing Impact of India's National Health Insurance Scheme (RSBY): Is There Any Evidence of Increased Health Care Utilisation? reached similar conclusions when tracking RSBY over time across multiple states, finding no real improvement in service utilisation and even declines in some areas
| [7] | Sinha, R. K., & Chatterjee, K. (2014). Assessing impact of India’s National health insurance scheme (RSBY): Is there any evidence of increased health care utilisation. International Journal of Humanities and Social Science, 4(5), 223-232. |
[7]
. Sriram and Khan (2020) in
Effect of health insurance program for the poor on out-of-pocket inpatient care cost in India: evidence from a nationally representative cross-sectional survey add another dimension by showing that while insurance increased hospitalisation rates among below-poverty-line families, it did not reduce what they actually paid or how long they stayed in hospitals.
| [6] | Sriram, S., & Khan, M. M. (2020). Effect of health insurance program for the poor on out-of-pocket inpatient care cost in India: evidence from a nationally representative cross-sectional survey. BMC Health Services Research, 20(1).
https://doi.org/10.1186/s12913-020-05692-7 |
[6]
The common thread across these studies is that current insurance schemes have serious structural flaws, particularly because they exclude outpatient care, which limits their effectiveness in providing real financial protection. Furthermore, administrative inefficiencies within the system further compound these inadequacies, with Mittal and Gupta (2023) in
The Problems and Challenges of Health Insurance in India noting that claim settlement delays have historically averaged 121 days, causing hospitals to withdraw cashless treatment facilities and further deterring utilisation among vulnerable populations.
| [8] | The Problems and Challenges of Health Insurance in India. (2023). International Journal for Research Trends and Innovation, 8(4), 267, 268, 269. https://www.ijrti.org/papers/IJRTI2304043.pdf |
| [21] | Mittal, A., & Gupta, N. (2023). The problems and challenges of health insurance in India. International Journal for Research Trends and Innovation, 8(4), 267–269. |
[8, 21]
.
Aside from financial constraints, behavioural and perceptual factors constitute substantive determinants of healthcare non-utilisation. A systematic review and meta-analysis (2025) in
Health-seeking behaviour and its determinants for non-communicable diseases in India identified the lack of disease awareness as a major reason for treatment delays
| [9] | Haridoss, M., Nandi, D., Rajesh Lenin, R., John, S. P., Anantharaman, V. V., & Janardhanan, R. (2025). Health-seeking behavior and its determinants for non-communicable diseases in India-a systematic review and meta-analysis. Frontiers in Public Health, 13, 1580824. |
[9]
. Even when symptoms appear, many people do not understand the long-term advantages of early intervention for conditions like hypertension or diabetes, so they simply do not seek care. The National Institution for Transforming India (2020) analysed three rounds of National Sample Survey data in
Morbidity, Health-Seeking Behaviour and Out-of-Pocket Expenditure among Large Indian States and found that most people skip medical consultations because they think their illness is not serious enough
| [10] | Ranganadham, S. (2022). Morbidity, Health-Seeking Behaviour and out-of-Pocket Expenditure among Large Indian States. New Delhi, India: NITI Aayog. |
[10]
. What is particularly striking is that in many regions, these behavioural barriers actually outweigh financial ones: people choose expensive private care over free or subsidised public services, suggesting that quality concerns matter more than cost in their decision-making. Kusuma and Babu (2019), in
The Costs of Seeking Healthcare: Illness, Treatment Seeking and Out-of-Pocket Expenditures among the Urban Poor in Delhi, India, found that perceived seriousness of illness was a key factor influencing whether individuals sought treatment
| [12] | Kusuma, Y. S., & Babu, B. V. (2019). The costs of seeking healthcare: Illness, treatment seeking and out of pocket expenditures among the urban poor in Delhi, India. Health & Social Care in the Community, 27(6), 1401-1420. |
[12]
. This suggests that individuals may be less likely to seek care for conditions they do not consider severe, potentially delaying timely medical intervention.
Gender constitutes a significant axis of healthcare utilisation inequality within the Indian context. Miller and colleagues (2023) used data from Rajasthan in
Women Left Behind: Gender Disparities in Utilisation of Government Health Insurance in India to show that even when government insurance makes healthcare theoretically "free," women, particularly young girls and elderly women, are far less likely than men to receive treatment
| [11] | Dupas, P., & Jain, R. (2021). Women Left Behind: Gender Disparities in Utilization of Government Health Insurance in. |
[11]
. They found that non-monetary costs like travel distance and unauthorised fees that healthcare providers charge create barriers that lead families to prioritise men's health over women's health. Kanuganti et al. (2015) in
Quantification of accessibility to health facilities in rural areas examined villages connected under the Pradhan Mantri Gram Sadak Yojana and discovered that building roads improved physical access to clinics, but without reliable public transportation, people still struggled to reach healthcare facilities
| [5] | Kanuganti, S., Sarkar, A. K., Singh, A. P., & Arkatkar, S. S. (2015). Quantification of accessibility to health facilities in rural areas. Case Studies on Transport Policy, 3(3), 311–320.
https://doi.org/10.1016/j.cstp.2014.08.004 |
[5]
. This infrastructure gap compounds the distance-related barriers that hit vulnerable groups hardest. Dalal and Dawad (2009) in
Non-utilisation of public healthcare facilities: examining the reasons through a national study of women in India found through national-level data that women avoid public hospitals not just because of cost, but because they view the quality as poor: long waits and substandard care for female patients
| [13] | Dalal, K., & Dawad, S. (2009). Non-utilization of public healthcare facilities: examining the reasons through a national study of women in India. Rural and remote health, 9(3), 1-10. |
[13]
. This creates a vicious cycle where women deliberately ignore health problems to avoid the disrespect they experience in public health facilities. A 2023 review in
Understanding Healthcare Avoidance among Elderly in India: Perceptions of Medical Expenditure as a Barrier to Hospital Treatment highlighted similar patterns among elderly populations, showing how fear of medical costs leads to care avoidance, delayed diagnoses, and worse health outcomes for vulnerable older adults
.
3. Data Description and Analysis
This study uses the National Health Survey (NHS) (2017-18), collected by the Ministry of Statistics and Programme Implementation (MoSPI), Government of India, data on household health such as healthcare utilisation, expenditures, insurance coverages, barriers etc. It is a nationally representative dataset covering 113,823 households across different states in India.
Table 1. Percentage of the Sample Not Utilising Healthcare Facilities During Illness, by Gender and Reported Reasons.
Reported Reasons | Male | Female |
Financial constraint | 8.54% | 7.78% |
No medical facility available nearby | 28.11% | 26.85% |
Lack of faith | 8.17% | 8.97% |
Ailment not considered serious | 17.80% | 18.35% |
Long waiting period | 0.41% | 0.50% |
Other reasons | 31.63% | 32.05% |
*Source: Authors’ computations using National Health Survey 2017-18
In
Table 1, the most prominent barrier for both males and females is the absence of a nearby medical facility, reported by 28.11% of males and 26.85% of females. Financial constraints, by contrast, account for only 8.54% of males and 7.78% of females, which are among the lowest reported barriers. "Ailment not considered serious" is cited by 17.80% of males and 18.35% of females, and the distribution across all categories is remarkably uniform between genders, with most categories differing by less than one percentage point.
The prominence of facility unavailability as the leading barrier is a critical finding, as it highlights non-utilisation as a structural deficit, where the absence of accessible infrastructure makes seeking care very difficult regardless of willingness or financial capacity. The high reporting of "ailment not considered serious" across both genders reinforces the pattern identified by Kusuma and Babu (2019), wherein perceived seriousness of illness shapes treatment-seeking behaviour, with individuals more likely to seek care only when conditions are considered severe. Perhaps most striking is that financial constraints rank among the lowest reported barriers, directly challenging the assumption that cost is the primary driver of non-utilisation in a developing economy like India. The near-complete gender uniformity across all barriers, while notable, may partly reflect underreporting of gender-specific experiences among women, as documented by Miller et al. (2023). Yet, the data as presented suggests that systemic barriers affect men and women in highly similar ways and that the barriers to entry for healthcare are systemic rather than gender-specific in this dataset.
The unavailability of facilities points to a structural supply-side gap that disproportionately disadvantages rural populations. The fact that even higher-educated individuals report facility unavailability as a reason for non-utilisation indicates that geographic inaccessibility is more of a systemic failure in healthcare infrastructure distribution, and not just a consequence of poverty or low awareness. This corroborates Kanuganti et al. (2015), who found physical inaccessibility to be a binding constraint on utilisation independent of other factors.
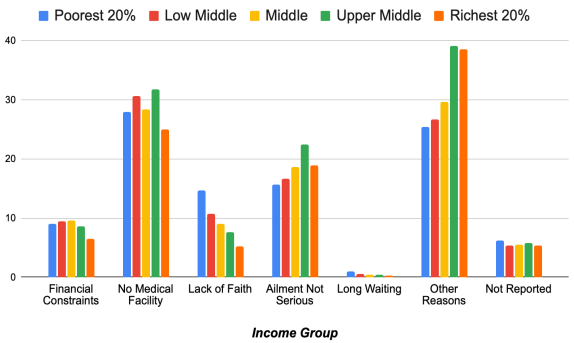
Figure 1. Percentage of the Sample Not Utilising Healthcare Facilities During Illness, by Wealth Quintile and Reported Reasons.
In
Figure 1, several distinct patterns are visible across the wealth quintiles, the most notable being that financial constraint as a barrier declines as wealth increases. The absence of a nearby medical facility remains the dominant reported barrier across all quintiles, ranging from 25.02% among the richest to 31.83% among the upper middle, and 27.97% among the poorest 20%: with no clear gradient, indicating that geographic inaccessibility is not a problem just for the poor. A more prominent gradient is visible in "lack of faith", which falls from 14.68% among the poorest to just 5.25% among the richest, which is nearly a threefold difference. Conversely, "ailment not considered serious" rises with wealth, from 15.71% among the poorest to 22.50% among the upper middle quintile, before slightly declining among the richest.
The near-flat distribution of financial constraints across quintiles is a striking observation as it suggests that cost is not the barrier that most sharply differentiates healthcare behaviour across income groups, reinforcing the finding from
Table 1 that financial constraints are a less dominant driver of non-utilisation than conventionally assumed. The steep decline in lack of faith with rising wealth points to a two-tiered healthcare experience, where wealthier households are likely to access better-equipped private facilities with qualified practitioners, while poorer households largely experience under-resourced public facilities, eroding their trust and deterring future utilisation, as documented by Dalal and Dawad (2009). The rise in "ailment not considered serious" with wealth is equally striking. Wealthier individuals, despite having greater financial capacity and better access to care, are more likely to dismiss their illness as insufficiently serious to warrant treatment, which suggests that the behavioural tendency to underestimate illness severity is not a consequence of poverty or low awareness, but persists and even intensifies across the income distribution. This has significant policy implications, as it indicates that improving access and affordability alone will not resolve non-utilisation if the underlying disposition to delay care remains unaddressed. Finally, the persistence of facility unavailability as the leading barrier across all wealth quintiles re-confirms that geographic inaccessibility is a systemic infrastructure failure regardless of the wealth quintile.
In
Table A1, the most pronounced cost differential observed in the data is between government and private hospitals. At the all-India level, average expenditure at government hospitals stands at Rs. 331 per spell, compared to Rs. 1,062 at private hospitals, which is more than three times higher. This disparity holds consistently across both rural and urban sectors. Urban patients incur higher expenditure across almost every provider category, with the aggregate urban average (Rs. 710) exceeding the rural average (Rs. 592), reflecting generally higher service costs in urban settings.
The fact that government hospitals are substantially cheaper than every other provider type, and yet patients demonstrably seek care elsewhere at considerably greater cost, indicates that financial considerations alone do not determine provider choice. The willingness to incur expenditure up to three times higher at private facilities suggests that perceived quality and reliability of public institutions play an independent role in determining where, and whether, individuals seek care. This situation where private care is unaffordable and public care is avoided, likely results in treatment being foregone altogether, directly contributing to non-utilization. Dalal and Dawad (2009) corroborate this, finding that poor perceived quality of public facilities was a significant reason individuals avoided them, while NITI Aayog (2020) similarly found that individuals frequently bypass subsidised public services in favour of costlier private alternatives. The expenditure patterns in this table therefore suggest that non-utilization in India is not driven purely by inability to pay, but by a combination of financial and quality-related barriers that together reduce the likelihood of treatment-seeking among vulnerable populations.
Table 2. Percentage of the Sample Not Utilising Healthcare Facilities During Illness, by Education Level and Reported Reasons.
Education | Financial Constraint | No medical facility available nearby | Lack of faith | Ailment not considered serious | Long waiting period | Other reasons |
Not Literate | 33.56% | 40.29% | 43.48% | 36.06% | 46.61% | 31.42% |
Primary | 14.13% | 12.32% | 16.50% | 13.63% | 11.86% | 15.25% |
Secondary | 29.64% | 25.33% | 23.74% | 26.79% | 23.73% | 27.65% |
Higher Education | 22.67% | 22.06% | 16.28% | 17.80% | 17.80% | 25.68% |
*Source: Authors’ computations using National Health Survey 2017-18
Table 3. Amount Reimbursed as a Percentage of Total Medical Expenses.
Type of Hospital | Amount reimbursed as% of total medical expenditure |
Quintile class of household expenditure |
1st | 2nd | 3rd | 4th | 5th | All |
rural |
Public | 3.9 | 1.1 | 6.4 | 1.9 | 8.7 | 5.1 |
Private | 1.9 | 1.4 | 2.5 | 5.2 | 6.1 | 4.4 |
All | 2.3 | 1.3 | 2.9 | 4.6 | 6.4 | 4.4 |
urban |
Public | 2.9 | 5.0 | 3.9 | 14.8 | 17.4 | 8.9 |
Private | 4.3 | 6.7 | 11.3 | 15.2 | 28.1 | 17.5 |
All | 4.0 | 7.8 | 10.7 | 15.1 | 26.9 | 16.8 |
*Source: Statement 3.19, National Health Survey 2017-18 Report
In
Table 2, the most striking observation is that illiteracy dominates non-utilisation across nearly every reported reason. The not-literate group records the highest percentages across all six categories, with long waiting periods (46.61%), lack of faith (43.48%), and no nearby facility (40.29%) being particularly prominent. However, what is significant is that behavioural barriers remain substantial even among the higher education group, at 39.80%.
In
Table 3, the reimbursement rates are uniformly low across all categories. In rural areas, the overall average stands at just 4.4%, while urban rates, though higher at 16.8%, remain deeply inadequate, which suggests that even the wealthiest urban quintile sees only 26.9% of medical costs reimbursed, meaning over 70% is paid out-of-pocket. A consistent pro-rich gradient is evident across both rural and urban areas, with reimbursement rising with income and the urban disparity being sharpest: the wealthiest quintile receives over six times the reimbursement of the poorest. It is visible that reimbursement rates at private hospitals tend to be higher than at public hospitals, but this advantage is concentrated among wealthier quintiles. Among the poorest households, this gap narrows or reverses, indicating that the insurance benefits at private facilities are largely captured by the higher-income groups, while the poorer households get minimal financial relief regardless of where they seek care.
These trends highlight a fundamental gap in health insurance acting as a financial safety net. For the poorest rural households, insurance recovers less than 3% of total medical expenditure, rendering it practically meaningless for the population it is supposedly designed to protect. This directly corroborates Prinja et al. (2019) and Sinha and Chatterjee (2014), who found no meaningful reduction in out-of-pocket expenditure attributable to insurance coverage. The administrative barriers identified by Mittal and Gupta (2023), including claim settlement delays averaging 121 days, further explain why reimbursement disproportionately benefits wealthier, urban households who are better equipped to handle these processes. Critically, when households anticipate negligible financial relief from insurance, the perceived cost of seeking care remains high, which reinforces the treatment-deferral behaviour documented throughout this study. Notably, even where the pro-rich gradient places wealthier households at an advantage, reimbursement rates remain far below what would provide meaningful financial protection, indicating that health insurance in its current form fails to provide the safety net it is intended to deliver across the income distribution.
4. Policy Recommendations
The critical issue of healthcare non-utilisation in India, despite the substantial investments and expansion of facilities, calls for a strategic re-evaluation of the policy interventions in place. Based on the barriers identified across the preceding analysis: geographic inaccessibility, behavioural dismissal of illness severity, erosion of institutional trust, and the failure of insurance to provide meaningful financial protection, this section gives targeted, evidence-based policy recommendations directed at reducing healthcare non-utilisation in India.
4.1. Strengthening Physical and Digital Healthcare Access
The most consistently reported barrier across all tables is the absence of a nearby medical facility, cutting across gender, wealth, and education groups alike. This demands a two-pronged response: physical infrastructure expansion and digital service delivery. The Pradhan Mantri Gram Sadak Yojana has improved road connectivity to rural areas, yet as Kanuganti et al. (2015) note, road access alone is insufficient without reliable transportation to healthcare facilities. A targeted extension of the scheme to subsidise last-mile patient transport, modelled on Kerala's patient transport scheme under the Emergency Medical Services programme, would meaningfully reduce the access gap for rural populations. Alongside this, the government should mandate the establishment of Sub-Health Centres (SHCs) within defined distance thresholds in underserved districts, with particular attention to regions where facility unavailability rates are highest.
On the digital front, the E-Sanjeevani telemedicine platform represents a significant step toward bridging geographic gaps, having facilitated millions of remote consultations since its launch
. However, its reach is constrained by low smartphone penetration and digital literacy in rural areas. Policy should therefore prioritise community-level digital access points, such as Common Service Centres, where trained facilitators assist rural populations in accessing telemedicine services, removing the technological barrier that currently limits uptake among precisely the populations who would benefit most.
4.2. Addressing Behavioural Barriers Through Awareness and Early Detection
The data consistently shows that a significant proportion of individuals across all demographic groups do not seek care because they do not consider their ailment serious — a pattern that is, paradoxically, more pronounced among wealthier quintiles. This points to the need for demand-side interventions targeting health literacy and illness awareness, not merely supply-side infrastructure investment. India's Ayushman Bharat Health and Wellness Centres provide an existing platform for community-level preventive care and awareness campaigns; these should be systematically strengthened to deliver structured screening programmes for high-burden non-communicable diseases such as hypertension, diabetes, and cancer, where the consequences of delayed diagnosis are most severe.
The Cancer Care application and similar condition-specific digital tools offer a promising model for early symptom identification and care navigation. Scaling such applications, paired with AI-driven diagnostic support systems of the kind piloted in Bihar
, where artificial intelligence was deployed to assist frontline health workers in identifying high-risk patients, could meaningfully shift the population's disposition from reactive to preventive care-seeking. Similar AI-assisted screening programmes have demonstrated efficacy in sub-Saharan Africa, where community health workers equipped with algorithm-supported diagnostic tools significantly improved early detection rates for tuberculosis and maternal health complications
. Replicating and scaling this model across India's Accredited Social Health Activist network would leverage an existing institutional infrastructure to deliver targeted behavioural nudges at the community level. As a developed country, Hong Kong has an eHealth app which allows public hospitals to upload individual public healthcare records
. India should accelerate the Ayushman Bharat Digital Mission (ABDM) to create a similar "Health Locker." This could be a centralized app which would store all public healthcare records. Like Hong Kong’s eHRSS, the app must allow private doctors at "Apollo-style" hospitals to see public clinic records, reducing the duplicate testing costs that currently drain household savings. This would reduce the higher costs spent on multiple tests in the same year. Furthermore, it could mean that some citizens can afford to travel farther to ensure that they receive the best care possible.
4.3. Reforming Health Insurance to More Efficiently Deliver Financial Protection
The analysis in this paper makes it clear that health insurance in its current form is failing as a financial safety net, with reimbursement rates as low as 2.3% for the poorest rural households. Structural reform is therefore essential. The most critical gap is the near-universal exclusion of outpatient care from existing insurance schemes, which Sriram and Khan (2020) identify as a primary reason why insurance fails to reduce out-of-pocket expenditure. Extending Ayushman Bharat PM-JAY coverage to include outpatient consultations, diagnostics, and medicines would address this gap directly, as hospitalisation costs, while catastrophic, represent only one dimension of the financial burden households bear.
Beyond coverage expansion, the administrative inefficiencies documented by Mittal and Gupta (2023), including claim settlement delays averaging 121 days, must be urgently addressed. Adopting a real-time digital claims processing system, as implemented under Thailand's Universal Coverage Scheme which achieved near-universal financial protection through streamlined cashless reimbursement
, would reduce the procedural burden that currently deters poorer and less administratively capable households from recovering insurance benefits. Additionally, the pronounced pro-rich gradient in reimbursement suggests that active outreach and claims facilitation support must be directed toward lower-income and rural beneficiaries who lack the capacity to navigate complex reimbursement processes independently.
4.4. Rebuilding Institutional Trust
To restore faith in the Indian population which currently deters nearly 15% of the poorest quintile from seeking care, a policy should focus on Quality Standardisation across India and transparency. Public facilities should contain dashboards which showcase doctor attendance, bed and room availability as well as medicines stocks. There should also be patient feedback loops where patients can fill in satisfaction forms which incentivise providers to deliver respectful and high-quality clinical care. This move toward a consumer-rights approach will help close the trust gap that separates the poorest 20% from the richest 20% of the population. Addressing this requires investment not only in physical infrastructure and equipment but in the patient experience, through accountability mechanisms, grievance redressal systems, and quality certification of public facilities.
5. Conclusion
Our study highlights that healthcare access and usage in India is primarily dependent on the intersection between geographical distance, economic status and a lack of faith which particularly affects the marginalised and rural communities. The data from the NSS 75th Round (2017-18) highlights that the avoidance of primary care results in extremely high hospitalisation rates, predominantly for women. Furthermore, the financial burdens are quite severe with medicines consuming around 82.2% of public health expenditure forcing around 13.4%
of rural households into debt which neutralises the benefits of the “free” or “heavily subsidized” healthcare. Hence, leading to the non-utilisation of healthcare until the severity of an ailment is undeniable.
Abbreviations
NHS | National Health Survey |
GHE | Government Health Expenditure |
RSBY | Rashtriya Swasthya Bima Yojana |
MoSPI | Ministry of Statistics and Programme Implementation |
SHCs | Sub-Health Centres |
ABDM | Ayushman Bharat Digital Mission |
Acknowledgments
We thank Dr. Pragati for her invaluable feedback and guidance throughout our research. We also acknowledge the resources provided by the John Nash Research Program, which significantly assisted with the timely completion of our paper.
Author Contributions
Vihaan Kenia: Conceptualization, Methodology, Data curation, Formal analysis, Writing – original draft, Writing – review & editing
Anya Motiwala: Conceptualization, Methodology, Data curation, Formal analysis, Writing – original draft, Validation, Writing – review & editing
Data Availability Statement
The data which supports the findings of this research are derived from the National Health Survey (NHS) 75th Round (2017-18) on household social consumption, with regards to health. It is collected by the Ministry of Statistics and Programme Implementation (MoSPI), Government of India. The unit-level data is publicly available and can be accessed through the Microdata Catalogue of the Government of India (https://microdata.gov.in/NADA/index.php/catalog/152). All of the analysed data integrated into the research results are available from the corresponding author upon a reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix
Table A1. Average Medical Expenditure Across Various Healthcare Facilities in India (in INR).
| Govt./ Public Hospitals | Private Hospitals | Trust/ NGO-run Hospitals | Private doctor/ Clinics | Informal Healthcare Providers | All |
Rural | 325 | 1,081 | 624 | 566 | 487 | 592 |
Urban | 344 | 1,038 | 863 | 714 | 1,035 | 710 |
All | 331 | 1,062 | 732 | 624 | 552 | 636 |
*Source: Authors’ curation from National Health Survey 2017-18 Report
Table A2. Percentage break-up of treated ailments by type of healthcare service provider, all-India.
Healthcare Service Provider | Percentage of treated ailments |
Rural | Urban | All |
Government/ Public Hospital | 32.5 | 26.2 | 30.1 |
Private Hospital | 20.8 | 27.3 | 23.3 |
Charitable/Trust/NGO-run Hospital | 0.9 | 1.3 | 1.1 |
Private Doctor / In Private Clinic | 41.4 | 44.3 | 42.5 |
Informal Health Care Provider | 4.3 | 0.9 | 3.0 |
All | 100.0 | 100.0 | 100.0 |
*Source: Authors’ curation from National Health Survey 2017-18 Report
Table A3. Percentage of the Sample Not Utilising Healthcare Facilities During Illness, by Wealth Quintile and Reported Reasons.
| Poorest 20% | Lower Middle | Middle | Upper Middle | Richest 20% |
Financial constraint | 9.10% | 9.39% | 9.61% | 8.56% | 6.54% |
No medical facility available nearby | 27.97% | 30.61% | 28.36% | 31.83% | 25.02% |
Lack of faith | 14.68% | 10.76% | 9.08% | 7.59% | 5.25% |
Ailment not considered serious | 15.71% | 16.65% | 18.69% | 22.50% | 18.95% |
Long waiting period | 0.94% | 0.56% | 0.35% | 0.41% | 0.28% |
Other reasons | 25.35% | 26.69% | 29.60% | 39.17% | 38.60% |
*Source: Authors’ computations using National Health Survey 2017-18
References
| [1] |
Ghosh S. (2014). Equity in the utilization of healthcare services in India: evidence from National Sample Survey. International journal of health policy and management, 2(1), 29–38.
https://doi.org/10.15171/ijhpm.2014.06
|
| [2] |
Prinja, S., Bahuguna, P., Gupta, I., Chowdhury, S., & Trivedi, M. (2019). Role of insurance in determining utilization of healthcare and financial risk protection in India. PloS one, 14(2), e0211793.
|
| [3] |
Purohit B. C. (2004). Inter-state disparities in health care and financial burden on the poor in India. Journal of health & social policy, 18(3), 37–60.
https://doi.org/10.1300/J045v18n03_03
|
| [4] |
Understanding Healthcare Avoidance among Elderly in India: Perceptions of Medical Expenditure as a Barrier to Hospital Treatment. (2023). Journal of Psychosocial Wellbeing, 4(1), 39-44.
https://jpsw.co.in/index.php/jpsw/article/view/106
|
| [5] |
Kanuganti, S., Sarkar, A. K., Singh, A. P., & Arkatkar, S. S. (2015). Quantification of accessibility to health facilities in rural areas. Case Studies on Transport Policy, 3(3), 311–320.
https://doi.org/10.1016/j.cstp.2014.08.004
|
| [6] |
Sriram, S., & Khan, M. M. (2020). Effect of health insurance program for the poor on out-of-pocket inpatient care cost in India: evidence from a nationally representative cross-sectional survey. BMC Health Services Research, 20(1).
https://doi.org/10.1186/s12913-020-05692-7
|
| [7] |
Sinha, R. K., & Chatterjee, K. (2014). Assessing impact of India’s National health insurance scheme (RSBY): Is there any evidence of increased health care utilisation. International Journal of Humanities and Social Science, 4(5), 223-232.
|
| [8] |
The Problems and Challenges of Health Insurance in India. (2023). International Journal for Research Trends and Innovation, 8(4), 267, 268, 269.
https://www.ijrti.org/papers/IJRTI2304043.pdf
|
| [9] |
Haridoss, M., Nandi, D., Rajesh Lenin, R., John, S. P., Anantharaman, V. V., & Janardhanan, R. (2025). Health-seeking behavior and its determinants for non-communicable diseases in India-a systematic review and meta-analysis. Frontiers in Public Health, 13, 1580824.
|
| [10] |
Ranganadham, S. (2022). Morbidity, Health-Seeking Behaviour and out-of-Pocket Expenditure among Large Indian States. New Delhi, India: NITI Aayog.
|
| [11] |
Dupas, P., & Jain, R. (2021). Women Left Behind: Gender Disparities in Utilization of Government Health Insurance in.
|
| [12] |
Kusuma, Y. S., & Babu, B. V. (2019). The costs of seeking healthcare: Illness, treatment seeking and out of pocket expenditures among the urban poor in Delhi, India. Health & Social Care in the Community, 27(6), 1401-1420.
|
| [13] |
Dalal, K., & Dawad, S. (2009). Non-utilization of public healthcare facilities: examining the reasons through a national study of women in India. Rural and remote health, 9(3), 1-10.
|
| [14] |
Press Information Burau, Government of India. National Health Account (NHA) Estimates 2020-21 and 2021-22. Available from:
https://www.pib.gov.in/PressNoteDetails.aspx?NoteId=153237&ModuleId=3®=3&lang=2
(accessed 16 May 2026).
|
| [15] |
Press Information Bureau, Government of India. Share of Government Health Expenditure in the Total Health Expenditure. Available from:
https://www.pib.gov.in/PressReleasePage.aspx?PRID=2097868®=3&lang=2
(accessed 16 May 2026).
|
| [16] |
Aulia Putri Pandamsari. (2023b, November 6). iClaim boosts Thailand’s health insurance claims in 10 seconds. Asian Business Review.
https://asianbusinessreview.com/exclusive/iclaim-boosts-thailands-health-insurance-claims-in-10-seconds
|
| [17] |
RW-Admin. (2025). AI making it easier to diagnose TB in sub-Saharan Africa. Stellenbosch University.
https://www.su.ac.za/en/node/20120
|
| [18] |
AI Revolutionizes TB Detection in Purnia, Bihar. (2023). Qure.ai.
https://www.qure.ai/impact-stories/AI-helps-overcome-healthcare-challenges-in-Bihar
|
| [19] |
eSanjeevani. (n.d.). Esanjeevani.mohfw.gov.in.
https://esanjeevani.mohfw.gov.in/#/
|
| [20] |
Health Bureau. (n.d.). eHealth - Home. eHealth System (Subsidies) Information. Retrieved March 19, 2026, from
https://www.ehealth.gov.hk/mobile-app
|
| [21] |
Mittal, A., & Gupta, N. (2023). The problems and challenges of health insurance in India. International Journal for Research Trends and Innovation, 8(4), 267–269.
|
| [22] |
National Statistical Office. (2019, November). Key indicators of social consumption in India: Health (NSS KI 75/25.0). Ministry of Statistics and Programme Implementation, Government of India.
https://www.mospi.gov.in/sites/default/files/publication_reports/KI_Health_75th_Final.pdf
|
Cite This Article
-
APA Style
Kenia, V., Motiwala, A. (2026). The Doctor Is There but the Patient Is Missing: Understanding Low Healthcare Utilisation in India. International Journal of Health Economics and Policy, 11(2), 111-120. https://doi.org/10.11648/j.hep.20261102.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Kenia, V.; Motiwala, A. The Doctor Is There but the Patient Is Missing: Understanding Low Healthcare Utilisation in India. Int. J. Health Econ. Policy 2026, 11(2), 111-120. doi: 10.11648/j.hep.20261102.15
Copy
|
Download
AMA Style
Kenia V, Motiwala A. The Doctor Is There but the Patient Is Missing: Understanding Low Healthcare Utilisation in India. Int J Health Econ Policy. 2026;11(2):111-120. doi: 10.11648/j.hep.20261102.15
Copy
|
Download
-
@article{10.11648/j.hep.20261102.15,
author = {Vihaan Kenia and Anya Motiwala},
title = {The Doctor Is There but the Patient Is Missing: Understanding Low Healthcare Utilisation in India},
journal = {International Journal of Health Economics and Policy},
volume = {11},
number = {2},
pages = {111-120},
doi = {10.11648/j.hep.20261102.15},
url = {https://doi.org/10.11648/j.hep.20261102.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.hep.20261102.15},
abstract = {This research pinpoints the multifaceted barriers that influence health-care seeking behaviour in India. It addresses a critical gap in understanding why a significant portion of the population are not utilising healthcare despite many national health initiatives. The main purpose of this study is to investigate how financial means, geographical inaccessibility and a lack of faith in the medical system intersect and ultimately lead to the deterrence of individuals from seeking necessary medical treatment or interventions. The study aims to provide actionable insights and policy recommendations to refine the public health strategy in India. Utilising the National Health Survey (2017-2018), the research analyses a sample of 113,823 households. The analysis reveals interesting findings - (a) the poorest 20% are nearly three times more likely to avoid care due to lack of faith in the medical facilities compared to the richest 20%; (b) geographical distance is a primary deterrent with 27% of the respondents citing there is a lack of a nearby medical facility, hence avoiding treatment till it is absolutely vital; (c) Despite availability of policies to reduce the burden of healthcare expenses such as PM-JAY, the financial burden still remains high for many. These results highlight that expanding insurance coverage is insufficient without investments in rural infrastructure and other initiatives to rebuild public trust in the healthcare system.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - The Doctor Is There but the Patient Is Missing: Understanding Low Healthcare Utilisation in India
AU - Vihaan Kenia
AU - Anya Motiwala
Y1 - 2026/05/30
PY - 2026
N1 - https://doi.org/10.11648/j.hep.20261102.15
DO - 10.11648/j.hep.20261102.15
T2 - International Journal of Health Economics and Policy
JF - International Journal of Health Economics and Policy
JO - International Journal of Health Economics and Policy
SP - 111
EP - 120
PB - Science Publishing Group
SN - 2578-9309
UR - https://doi.org/10.11648/j.hep.20261102.15
AB - This research pinpoints the multifaceted barriers that influence health-care seeking behaviour in India. It addresses a critical gap in understanding why a significant portion of the population are not utilising healthcare despite many national health initiatives. The main purpose of this study is to investigate how financial means, geographical inaccessibility and a lack of faith in the medical system intersect and ultimately lead to the deterrence of individuals from seeking necessary medical treatment or interventions. The study aims to provide actionable insights and policy recommendations to refine the public health strategy in India. Utilising the National Health Survey (2017-2018), the research analyses a sample of 113,823 households. The analysis reveals interesting findings - (a) the poorest 20% are nearly three times more likely to avoid care due to lack of faith in the medical facilities compared to the richest 20%; (b) geographical distance is a primary deterrent with 27% of the respondents citing there is a lack of a nearby medical facility, hence avoiding treatment till it is absolutely vital; (c) Despite availability of policies to reduce the burden of healthcare expenses such as PM-JAY, the financial burden still remains high for many. These results highlight that expanding insurance coverage is insufficient without investments in rural infrastructure and other initiatives to rebuild public trust in the healthcare system.
VL - 11
IS - 2
ER -
Copy
|
Download