Introduction: Trachoma, caused by the bacterium Chlamydia trachomatis, remains a significant public health concern and the leading infectious cause of blindness worldwide. In 2021, trachoma was endemic in 42 countries, primarily located in Africa, and accounted for 80% of the global burden of blindness due to an infectious disease. Despite the availability of effective prevention strategies and treatment, trachoma continues to be a major issue in certain regions, including Ethiopia. Objectives: This study aimed to assess the prevalence and identify factors associated with trachoma among children aged 1-9 years in rural communities of the Kombolcha district, East Hararge zone, Oromia Regional State, Ethiopia. Methods: A cross-sectional study design was employed, involving children aged 1-9 years in rural communities. A multistage random sampling method was utilized to select 622 study participants. Data were collected through face-to-face interviews using a structured questionnaire, which was pretested on 5% of the sample size. After data cleaning and entry into Epi Info version 7.1, data were exported to SPSS version 23 for analysis. Variables with a p-value < 0.20 in bivariate binary logistic regression were included in a multivariate binary logistic regression model to identify factors associated with trachoma. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated to evaluate the strength of associations at a p-value < 0.05. Results: The overall prevalence of active trachoma among children aged 1-9 years was 7.55%. Of the affected children, 83% exhibited trachomatous inflammation follicular (TF), 11% had trachomatous inflammation intense (TI), and 6% had both TF and TI. The prevalence ranged from 2.7% in children aged 1-4 years to 10.4% in children aged 5-9 years. In the multivariate analysis, factors significantly associated with the presence of active trachoma in the study population included: * Households with unprotected water sources (AOR = 0.32, 95% CI: 0.15-0.67) * Regular towel usage (AOR = 8.03, 95% CI: 2.18-29.6) * Not using soap to wash the face (AOR = 4.53, 95% CI: 2.13-9.63) * Family history of eye problems (AOR = 4.76, 95% CI: 2.19-10.35) Conclusion and Recommendation: The overall prevalence of active trachoma in the study area was 7.55%. While this prevalence is below the WHO threshold for mass drug administration (MDA) (>10%), it remains a significant public health concern. The findings highlight the need to implement the WHO-endorsed SAFE strategy, which focuses on surgery, antibiotics, facial cleanliness, and environmental improvement, to effectively prevent and control trachoma. Additionally, improving the overall living conditions of the community through coordinated efforts is essential in addressing the factors associated with the disease.
| Published in | International Journal of Health Economics and Policy (Volume 9, Issue 3) |
| DOI | 10.11648/j.hep.20240903.11 |
| Page(s) | 57-70 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Associated Factor, Children Aged 1-9 Years, Kombolcha District, Prevalence, Trachoma
Factors considered | Proportion –value | Sample | OR | Calculated sample size | Reference |
|---|---|---|---|---|---|
Unclean face | % of cases in children who have no unclean face =42%. | 224 | 2.4 | 338 | (27) |
% of cases in children who have unclean face =58%. | |||||
Not have functional latrine | % of cases in children, HH who have not functional latrine=40%. | 26 | 4.39 | 214 | (28) |
% of cases in children, HH who have functional latrine =9.2%. | |||||
Waste around house | % of cases where no waste around house =53.8%. % of case where have waste around house=68.5%. | 374 | 1.68 | 622 | (6) |
characteristics | Categories | Frequency (n) | Percentage (%) |
|---|---|---|---|
Sex of the children | Male | 275 | 44.2 |
Female | 347 | 55.8 | |
Age of the children | 1-4 year | 222 | 35.7 |
≥5 year | 400 | 64.3 | |
Ethnicity | Amhara | 25 | 4.0 |
Oromo | 594 | 95.5 | |
Others# | 3 | 0.5 | |
Religion | Muslim | 602 | 96.8 |
Orthodox | 20 | 3.2 | |
Educational status of the child | Enrolled at school | 125 | 20.1 |
Not enrolled at school | 497 | 79.9 |
Variables | Category | NTR | TR | χ2 |
|---|---|---|---|---|
N (%) | N (%) | |||
Mother’s Educational level | Unable to read and write | 295 (51.3%) | 32 (68.1%) | 0.263 |
Able to read and write | 175 (30.4%) | 9 (19.1%) | ||
Primary education. | 98 (17%) | 6 (12.8%) | ||
Secondary education | 6 (1%) | 0 (0%) | ||
College and above | 1 (0.2%) | 0 (0%) | ||
Total | 575 (100%) | 47 (100%) | ||
HH’s Occupation | Farmer. | 494 (85.9%) | 39 (83%) | 0.002*** |
Merchant | 23 (4%) | 1 (2.1%) | ||
Employed | 5 (0.9%) | 0 (0%) | ||
Daily Lobar | 9 (1.6%) | 5 (10.6%) | ||
Both farmers & merchant | 44 (7.7%) | 2 (4.3%) | ||
Total | 575 (100%) | 47 (100%) | ||
HH’s Monthly Income (Birr) | ≤2500 | 566 (98.4%) | 46 (97.9%) | 0.768 |
>2500 | 9 (1.6%) | 1 (2.1%) | ||
Total | 575 (100%) | 47 (100%) |
Characteristics | NTR N. (%) | TR N. (%) | COR (95% CI) | P-Value | |
|---|---|---|---|---|---|
Child’s Sex | Male | 257 (93.5) | 18 (6.5) | 1 | |
Female | 318 (91.6) | 29 (8.4) | 1.8 (0.84 -3.83) | 0.135 | |
Child’s Age | 1-4 year | 216 (97.35) | 6 (27) | 1 | |
≥ 5 years | 359 (89.8) | 41 (10.3) | 2.6 (1.0 - 6.62) | 0.049 | |
Water source | Protected | 493 (95.4) | 24 (4.6) | 1 | |
Unprotected | 82 (78.1) | 23 (21.9) | 2.8 (1.32 - 6.1) | 0.008 | |
Hygienic condition of the child's face | Clean | 467 (95.3) | 23 (4.7) | 1 | |
Unclean | 108 (81.8) | 24 (18.2) | 1.55 (0.71 - 3.4) | 0.28 | |
Towel usage | Common | 5 (26.3.) | 14 (73.7) | 1 | |
None | 570 (94.5) | 33 (5.5) | 0.12 (0.03 - 0.47) | 0.002 | |
Washing face by soap | No | 144 (80.9) | 34 (19.1) | 1 | |
Yes | 431 (97.1) | 13 (2.9) | 0.3 (0.12 - 0.81) | 0.02 | |
Eye problem in family | Present | 65 (71.4) | 26 (28.6) | 1 | |
Absent | 510 (96) | 21 (4) | 0.24 (0.12 - 0.53) | 0.000 | |
Family Size | ≤4 | 358 (93.7) | 24 (6.3) | 1 | |
≥5 | 217 (90.4) | 23 (9.6) | 1.24 (0.59-2.59) | 0.56 | |
Face Washing frequency | ≤ once a day | 290 (87.6) | 41 (12.4) | ||
≥ once a day | 285 (97.9) | 6 (2.1) | 0.66 (0.21-2.13) | 0.49 | |
Characteristics | NTR (N. (%)) | TR (N. (%)) | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|---|
Child’s Sex | Male | 257 (93.5) | 18 (6.5) | 1 | 0.56 (0.26-1.18) |
Female | 318 (91.6) | 29 (8.4) | 1.8 (0.84 -3.83) | 1 | |
Child’s Age | 1-4 year | 216 (97.35) | 6 (27) | 1 | 0.39 (0.16-1.02) |
≥ 5 years | 359 (89.8) | 41 (10.3) | 2.6 (1.0 - 6.62) | 1 | |
Water source | Protected | 493 (95.4) | 24 (4.6) | 1 | 0.32 (0.15- 0.67) ** |
Unprotected | 82 (78.1) | 23 (21.9) | 2.8 (1.32 - 6.1) | 1 | |
Towel usage | Common | 5 (26.3.) | 14 (73.7) | 1 | 8.03 (2.18-29.6)** |
None | 570 (94.5) | 33 (5.5) | 0.12 (0.03 - 0.47) | 1 | |
wash face by soap | No | 144 (80.9) | 34 (19.1) | 1 | 4.53 (2.13-9.63)*** |
Yes | 431 (97.1) | 13 (2.9) | 0.3 (0.12 - 0.81) | 1 | |
Eye problem in family | Present | 65 (71.4) | 26 (28.6) | 1 | 4.76 (2.19-10.35)*** |
Absent | 510 (96) | 21 (4) | 0.24 (0.12 - 0.53) | 1 | |
AKT | Abdurehman Kelu Tololu |
AOR | Adjusted Odds Ratio |
AHT | Addis Hordofa Tekle |
CI | Confidence Interval |
MTA | Melese Tadesse Aredo |
NGO | None Governmental Organization |
SNNPR | Southern Nations, Nationalities, and Peoples |
SPSS | Statistical Package for Social Sciences |
TAM | Taha Adem Mume |
TF | Trachomatous Inflammation Follicular |
TI | Trachomatous Inflammation |
TKB | Teresa Kissi Beyen |
TT | Trachomatous Trichiasis |
WHO | World Health Organization |
| [1] | Geneva WH orgaNizatioN. Global Elimination of Blinding Trachoma by the year 2020 L ’ Alliance OMS pour l ’ élimination mondiale du trachome cécitant d ’ ici l ’ an 2020. Wkly Epidemiol Rec. 2014; 39(26): 614–8. |
| [2] | Gedefaw M, Shiferaw A, Alamrew Z, Feleke A, Fentie T, Atnafu K. Current state of active trachoma among elementary school students in the context of ambitious national growth plan: the case of Ethiopia. Health (Irvine Calif) [Internet]. 2013; 5. Available from: |
| [3] | Mohamud MA. Knowledge on Trachoma among Visitors of A Selected Hospital in Dharkeynley District, Somalia SUBMITTED BY: SUBMITTED TO: Dr. ABM Alauddin Chowdhury. 2017; 1–53. |
| [4] | Trachoma A, Report S. Australian Trachoma Surveillance Report 2017. Vol. 16. 2016. |
| [5] | Global DL, Policy H, Sc M. Global Elimination of Blinding Trachoma by 2020: Is Ethiopia on track? Vol. 70. 2020. |
| [6] | Gross LL. Walden University This is to certify that the doctoral dissertation by. 2019. |
| [7] | Devereau NS. “If students know about trachoma, they will teach their families:” Turning to students and teachers in Amhara, Ethiopia to promote Facial cleanliness and Environmental improvement By Nicole S. Devereaux Hubert Department of Global Health Karen L. An. 2017. |
| [8] | Surveys T, Date S, Time S, Location S, Description S, Diseases NT, et al. COR-NTD, New Orleans, 2018 Breakout Session 2E COR-NTD, New Orleans,. 2018. |
| [9] | King JD, Ngondi J, Amnie A, Cromwell E. Trachoma among children in community surveys from four African Countries and implications of using school surveys for evaluating prevalence Trachoma among children in community surveys from four African countries and implications of using school surveys f. Int Heal •. 2013; 5 (March 2017): 280–7. |
| [10] | WHO. Trachoma Data From World Health Organization Alliance for the Global Elimination of Blinding Trachoma, Twelfth Meeting Geneva, Switzerland. 2008; 1(8): 42–6. |
| [11] | Masesa DE, Moshiro C, Masanja H, Mkocha H, Ngirwamungu E, Kilima P et al. Prevalence of active trachoma in Tanzania.. East Afr J Ophthalmol. 2007; 34(13): 211–5. |
| [12] | The OF, Alliance WHO, Global THE, Of E. BLINDING. 2013; (April): 22–4. |
| [13] | Organization WH. Report of the 4th global scientific meeting on trachoma. 2018; (November): 27–9. |
| [14] | Tesfaledet Tsegay, Yewulshet Mengistu. Application of Ordinal Logistic Regression Analysis in Determining Risk Factors of Active Trachoma among Rural Children of Aged 1-9 Years Old in Kaffa Zone, South West. ARC J Public Heal Community Med. 2019; 4(1): 20–8. |
| [15] | Asres M, Endeshaw M, Yeshambaw M. iMedPub Journals Prevalence and Risk Factors of Active Trachoma among Children in Gondar Zuria District North Gondar, Ethiopia Keywords: Study design. 2016; 1–9. |
| [16] | Latino-americana L, Pr HM, Sp MM, Sp NK, Augusto R, Guedes P, et al. w Só fazemos melhor aquilo que repetidamente insistimos em melhorar... w Efficacy and safety of endothelial keratoplasty: a systematic review and meta-analysis w Contact lenses as drug controlled release systems. A narrative review w Orbital apocrine hidr. 2016; 75. |
| [17] | Harding-esch EM, Kadimpeul J, Sarr B, Sane A, Badji S, Laye M, et al. Population-based prevalence survey of follicular trachoma and trachomatous trichiasis in the Casamance region of Senegal. 2018; 1–11. |
| [18] | Solomon AW, Pavluck AL, Courtright P, Aboe A, Adamu L, Alemayehu W, et al. The Global Trachoma Mapping Project: Methodology of a 34-Country Population-Based Study. Licens by Inf Healthc USA. 2015; 6586: 214–25. |
| [19] | Sydney U, Collaborating WHO. Australian Trachoma Surveillance Report 2017. 2018. |
| [20] | Sector H, Plan T. Health Sector Transformation Plan. |
| [21] |
Adera TH, Macleod C, Endriyas M, Dejene M, Willis R, BChu BK. Prevalence of and risk factors for trachoma in southern nations, nationalities, and peoples’ region, Ethiopia: results of 40 population-
based prevalence surveys carried out with the global trachoma mapping project. Ophthalmic Epidemiol [Internet]. 2016; 23(51): 84–93. Available from: https://doi.org/10.1080/09286586.2016.1247876 |
| [22] | Palmer SL, Winskell K, Patterson AE, Boubacar K, Ibrahim F, Namata I, et al. “A living death”: A qualitative assessment of quality of life among women with trichiasis in rural Niger. Int Health. 2014; 6(4): 291–7. |
| [23] | Grey THE. INTERVENTIONS TO IMPROVE FACIAL CLEANLINESS & ENVIRONMENTAL IMPROVEMENT FOR TRACHOMA PREVENTION AND CONTROL. Rev F E grey Lit. 2017. |
| [24] | Zambrano AI, Mu BE, Mkocha H, West SK. Exposure to an Indoor Cooking Fire and Risk of Trachoma in Children of Kongwa,. 2015; 1–10. |
| [25] | Solomon AW, Pavluck A, Courtright P et al., Adamu L, Dejene M, Mekasha A, Jemal ZH, Yadeta D, et al. PThe Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol [Internet]. 2015; 22(6): 214–225. Available from: |
| [26] | Meseret E. ORIGINAL ARTICLE RAPID TRACHOMA ASSESSMENT IN KERSA DISTRICT, SOUTHWEST ETHIOPIA. 2003; (7). |
| [27] | Zone GG, Gesesew H. Prevalence and factors associated with trachoma among children aged 1 – 9 years in Zala district,. 2016; 1663–70. |
| [28] | Alemayehu M, Koye DN, Tariku A, Yimam K. Prevalence of Active Trachoma and Its Associated Factors among Rural and Urban Children in Dera Woreda, Northwest Ethiopia: A Comparative Cross-Sectional Study, 2015. |
| [29] | Of N, Collaborating WHO, For C. Network of who collaborating centres for. 2016; (June). |
| [30] | Berhane Y, Worku A, Bejiga A, Adamu L, Alemayehu W, Bedri A. Prevalence of Trachoma in Ethiopia. Ethiop J Heal Dev. 2007; 21. |
| [31] | Adane N, Berhe R, Gedefaw M. Prevalence and associated factors of active trachoma among children aged 1–9 years in rural communities of Gonji Kolella district, west Gojjam zone, North West Ethiopia. BMC Res Notes [Internet]. 2015; 8. Available from: |
| [32] | Anteneh ZA, Getu WY. Prevalence of active trachoma and associated risk factors among children in Gazegibela district of Wagehemra Zone, Amhara region, Ethiopia: community-based cross-sectional study. Trop Dis Travel Med Vaccines [Internet]. 2016; 1–7. Available from: |
| [33] | Gebre T, Bailey R, Emerson P. IS ETHIOPIA ON TRACK TO ACHIEVING THE GLOBAL GOAL OF ELIMINAT- ING TRACHOMA AS A PUBLIC HEALTH PROBLEM BY 2020? 2020; 55: 33–44. |
| [34] | Mpyet C, Goyol M, Ogoshi C. Personal and environmental risk factors for active trachoma in children in Yobe state, North-Eastern Nigeria. Trop Med Int Heal [Internet]. 2010; 15. Available from: |
| [35] | Assefa N, Roba AA, Ahmed TA, Birmeka JK, Zergaw ED. Prevalence and Factors Associated with Trachoma among Primary School Children in Harari Region, Eastern Ethiopia. 2017; 7(3): 1–9. |
| [36] | Smith L, Rebecca M PJ. The geographical distribution and burden of trachoma in Africa. PLOS Neg Trop Dis. 2013; 7(2359): 1300–3. |
| [37] | Kassim K, Kassim J, Aman R, Abduku M, Tegegne M. Prevalence of active trachoma and associated risk factors among children of the pastoralist population in Madda Walabu rural district, Southeast Ethiopia: a community-based cross-sectional study. 2019; 5–11. |
| [38] | Tadesse A, Worku A, Kumie A, Yimer SA, Beselam T. The burden of and risk factors for active trachoma in the north and south Wollo zones of Amhara region, Ethiopia. Infect Dis Poverty [Internet]. 2017; 6. Available from: |
APA Style
Mume, T. A., Aredo, M. T., Tololu, A. K., Beyen, T. K., Tekle, A. H., et al. (2024). Prevalence of Trachoma and Associated Factors among Children Aged 1–9 Years in Kombolcha District, East Hararge, Oromiya Regional State, Ethiopia, 2021. International Journal of Health Economics and Policy, 9(3), 57-70. https://doi.org/10.11648/j.hep.20240903.11
ACS Style
Mume, T. A.; Aredo, M. T.; Tololu, A. K.; Beyen, T. K.; Tekle, A. H., et al. Prevalence of Trachoma and Associated Factors among Children Aged 1–9 Years in Kombolcha District, East Hararge, Oromiya Regional State, Ethiopia, 2021. Int. J. Health Econ. Policy 2024, 9(3), 57-70. doi: 10.11648/j.hep.20240903.11
AMA Style
Mume TA, Aredo MT, Tololu AK, Beyen TK, Tekle AH, et al. Prevalence of Trachoma and Associated Factors among Children Aged 1–9 Years in Kombolcha District, East Hararge, Oromiya Regional State, Ethiopia, 2021. Int J Health Econ Policy. 2024;9(3):57-70. doi: 10.11648/j.hep.20240903.11
@article{10.11648/j.hep.20240903.11,
author = {Taha Adem Mume and Melese Tadesse Aredo and Abdurehman Kelu Tololu and Teresa Kissi Beyen and Addis Hordofa Tekle and Dida Batu},
title = {Prevalence of Trachoma and Associated Factors among Children Aged 1–9 Years in Kombolcha District, East Hararge, Oromiya Regional State, Ethiopia, 2021
},
journal = {International Journal of Health Economics and Policy},
volume = {9},
number = {3},
pages = {57-70},
doi = {10.11648/j.hep.20240903.11},
url = {https://doi.org/10.11648/j.hep.20240903.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.hep.20240903.11},
abstract = {Introduction: Trachoma, caused by the bacterium Chlamydia trachomatis, remains a significant public health concern and the leading infectious cause of blindness worldwide. In 2021, trachoma was endemic in 42 countries, primarily located in Africa, and accounted for 80% of the global burden of blindness due to an infectious disease. Despite the availability of effective prevention strategies and treatment, trachoma continues to be a major issue in certain regions, including Ethiopia. Objectives: This study aimed to assess the prevalence and identify factors associated with trachoma among children aged 1-9 years in rural communities of the Kombolcha district, East Hararge zone, Oromia Regional State, Ethiopia. Methods: A cross-sectional study design was employed, involving children aged 1-9 years in rural communities. A multistage random sampling method was utilized to select 622 study participants. Data were collected through face-to-face interviews using a structured questionnaire, which was pretested on 5% of the sample size. After data cleaning and entry into Epi Info version 7.1, data were exported to SPSS version 23 for analysis. Variables with a p-value Results: The overall prevalence of active trachoma among children aged 1-9 years was 7.55%. Of the affected children, 83% exhibited trachomatous inflammation follicular (TF), 11% had trachomatous inflammation intense (TI), and 6% had both TF and TI. The prevalence ranged from 2.7% in children aged 1-4 years to 10.4% in children aged 5-9 years. In the multivariate analysis, factors significantly associated with the presence of active trachoma in the study population included: * Households with unprotected water sources (AOR = 0.32, 95% CI: 0.15-0.67) * Regular towel usage (AOR = 8.03, 95% CI: 2.18-29.6) * Not using soap to wash the face (AOR = 4.53, 95% CI: 2.13-9.63) * Family history of eye problems (AOR = 4.76, 95% CI: 2.19-10.35) Conclusion and Recommendation: The overall prevalence of active trachoma in the study area was 7.55%. While this prevalence is below the WHO threshold for mass drug administration (MDA) (>10%), it remains a significant public health concern. The findings highlight the need to implement the WHO-endorsed SAFE strategy, which focuses on surgery, antibiotics, facial cleanliness, and environmental improvement, to effectively prevent and control trachoma. Additionally, improving the overall living conditions of the community through coordinated efforts is essential in addressing the factors associated with the disease.
},
year = {2024}
}
TY - JOUR T1 - Prevalence of Trachoma and Associated Factors among Children Aged 1–9 Years in Kombolcha District, East Hararge, Oromiya Regional State, Ethiopia, 2021 AU - Taha Adem Mume AU - Melese Tadesse Aredo AU - Abdurehman Kelu Tololu AU - Teresa Kissi Beyen AU - Addis Hordofa Tekle AU - Dida Batu Y1 - 2024/08/30 PY - 2024 N1 - https://doi.org/10.11648/j.hep.20240903.11 DO - 10.11648/j.hep.20240903.11 T2 - International Journal of Health Economics and Policy JF - International Journal of Health Economics and Policy JO - International Journal of Health Economics and Policy SP - 57 EP - 70 PB - Science Publishing Group SN - 2578-9309 UR - https://doi.org/10.11648/j.hep.20240903.11 AB - Introduction: Trachoma, caused by the bacterium Chlamydia trachomatis, remains a significant public health concern and the leading infectious cause of blindness worldwide. In 2021, trachoma was endemic in 42 countries, primarily located in Africa, and accounted for 80% of the global burden of blindness due to an infectious disease. Despite the availability of effective prevention strategies and treatment, trachoma continues to be a major issue in certain regions, including Ethiopia. Objectives: This study aimed to assess the prevalence and identify factors associated with trachoma among children aged 1-9 years in rural communities of the Kombolcha district, East Hararge zone, Oromia Regional State, Ethiopia. Methods: A cross-sectional study design was employed, involving children aged 1-9 years in rural communities. A multistage random sampling method was utilized to select 622 study participants. Data were collected through face-to-face interviews using a structured questionnaire, which was pretested on 5% of the sample size. After data cleaning and entry into Epi Info version 7.1, data were exported to SPSS version 23 for analysis. Variables with a p-value Results: The overall prevalence of active trachoma among children aged 1-9 years was 7.55%. Of the affected children, 83% exhibited trachomatous inflammation follicular (TF), 11% had trachomatous inflammation intense (TI), and 6% had both TF and TI. The prevalence ranged from 2.7% in children aged 1-4 years to 10.4% in children aged 5-9 years. In the multivariate analysis, factors significantly associated with the presence of active trachoma in the study population included: * Households with unprotected water sources (AOR = 0.32, 95% CI: 0.15-0.67) * Regular towel usage (AOR = 8.03, 95% CI: 2.18-29.6) * Not using soap to wash the face (AOR = 4.53, 95% CI: 2.13-9.63) * Family history of eye problems (AOR = 4.76, 95% CI: 2.19-10.35) Conclusion and Recommendation: The overall prevalence of active trachoma in the study area was 7.55%. While this prevalence is below the WHO threshold for mass drug administration (MDA) (>10%), it remains a significant public health concern. The findings highlight the need to implement the WHO-endorsed SAFE strategy, which focuses on surgery, antibiotics, facial cleanliness, and environmental improvement, to effectively prevent and control trachoma. Additionally, improving the overall living conditions of the community through coordinated efforts is essential in addressing the factors associated with the disease. VL - 9 IS - 3 ER -
Department of Public Health, College of Health Science, Arsi University, Asella City, Ethiopia
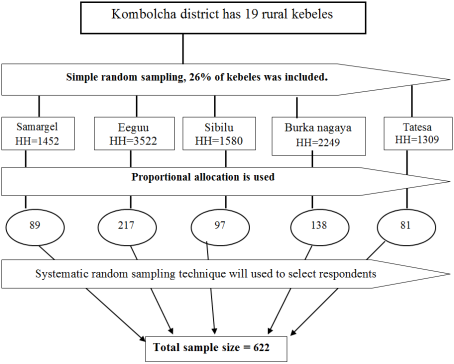
Figure 1. Schematic representation of the sampling method to assess prevalence of trachoma and associated factors among children aged 1– 9 years in rural communities of komolcha district.
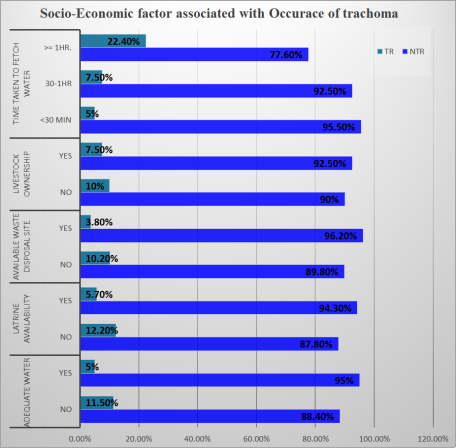
Figure 2. Socio-Economic factors associated with the occurrence of trachoma in Kombolcha district, Southeast Ethiopia, December 2021 (n =622).
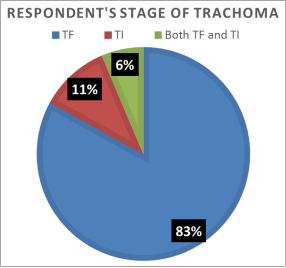
Figure 3. Respondent’s Stage of trachoma in Kombolcha district, South east Ethiopia, December, 2021 (n=47).
Information

